
From recollection to reality
Editor's note: Lynn Welsh is chief research officer at Olson Research Group. Tamara Fraley is client partner at PharmaACE.
Capturing real-world data in marketing research can be a powerful tool. When researching physician behavior, this technique extends beyond what can be measured in studies such as ATUs, where physicians report what they think or recall of their prescribing activity, since, whether subconsciously or consciously, when respondents of any type are asked to recall past behaviors there is an inherent risk of inaccuracy. With physicians, they may misremember their activity or portray their prescribing as more cutting-edge than it is, perhaps intuiting that reporting use of newer products on the market may be more interesting to the research sponsor.
With a chart audit study, we instruct physicians to select a sample of their recent patient charts that meet a specific criterion. Physicians are asked to input specific metrics from each chart into our survey platform, excluding any personally identifying information. While this forms the basis of what we are collecting in this research, chart studies can extend further by asking physicians clarifying questions around the chart data to illuminate the rationale behind prescribing decisions. For example, once objective measurements from the chart have been entered, follow-up questions can include: Why was this product selected for this patient? What other alternatives did you consider?
It is primarily for these reasons that chart research has the capacity to deliver timely, real-world prescribing activity combined with the reasons or factors at play in physician decision-making.
Understand the treatment landscape
Chart audit research is a tool for brand teams looking to launch and track their product or drug in the marketplace. Effective product launch and subsequent tracking requires examination of real-world data to accurately understand and evaluate the nuances of the competitive landscape. This can begin pre-launch to understand the treatment landscape prior to a new product’s availability and continue as the product is introduced, begins to see traction and eventually becomes a mature offering.
In addition to collecting actual treatment information (as opposed to treatment recall) chart audits let us attach patient demographics to treatment decisions. This allows brand teams to more clearly understand the specific type of patient (age, gender, comorbidities) for which their product is most often prescribed. Equally as important, teams can see this same information for competitive products as well, providing clarity beyond what can be gained by other sources of data.
Similarly, chart data can map the treatment progression landscape. With real-world chart data, brands can begin to understand what is typically prescribed before and after their product and in what specific patient circumstances. This allows the plotting of treatment progression, layering on varying patient characteristics to understand where patients normally come from in terms of treatment and where drug makers may be losing patients after they have tried their product.
While attaching patient demographics to treatment decisions affords a deeper understanding of prescribing behavior, a properly designed chart audit also allows for profiling at the HCP as well as the patient level. Physician demographics attached to prescribing choices highlight commonalities and differences between prescribers. Such data helps sales teams more effectively connect with physicians based on these nuances.
Further assess market share
With this understanding of the usefulness of adding chart audit research to the toolbox, it is important to examine the marketing utility of this methodology. Specifically, how does chart research help inform decision-making? First, by comparing what is learned from chart auditing, researchers can elaborate on information collected from third-party data. We can answer questions that might stem from what is learned with secondary data – for example, I can see my product’s market share overall but how does this share break out by type of patient? In short, chart data allows brands to further assess their market share by metrics relating to patient type, HCP type or other treatment or disease state indicators.
Second, by shedding light on treatment progression and sequencing, chart audit research can give brand teams a richer understanding of the prescribing habits of physicians. This information can be leveraged to develop messaging that better resonates with prescribers and offers deeper insight into treatment decisions and behavior. By extrapolating patient types, brand teams understand which patient factors most play a role in treatment decisions. Armed with this knowledge, clients can leverage those elements that best drive prescribing in sales and collateral messaging with their physicians. Finally, with the ability to identify and track prescribing trends, chart research can help ensure that marketing tactics are yielding results and can track changes in the competitive landscape, both as new products are introduced to a prescribing environment and older products mature out.
Methodological limitations
The above speaks to the potential of chart research to advance a brand team’s understanding of their competitive landscape. However, as with any methodology, chart research has limitations. There are key pitfalls to chart research and while these limitations are inevitable, articulating them at the outset helps to appropriately frame chart audits for clients.
First among the limitations is that physician participation in chart research is limited. Our internal research shows that, among physicians who are amenable to marketing research participation, roughly one-third are open to participating in chart audit research. This smaller respondent pool may result in a discrepancy in metrics that are commonly tracked in other forms of primary research. Thus, to be most effective, chart audit data must be assessed in conjunction with other data sources. However, what chart audit data may not fully deliver in alignment with other sources, it makes up for in the deeper insight into prescribing behavior that it can provide.
Second, variance in product share data is not uncommon; when comparing market share seen in chart research with that of other sources, there is often a distortion. The reasons behind this are twofold, due to the difference in sample makeup as explained above and the fact that it can be challenging to ensure that the sample, qualification process and data types collected are sufficiently comparable across different study methodologies. This can be accounted for when performing data triangulation or comparison of data across sources.
The final limitation to chart audit research is its inherent selection bias. While physicians are instructed as to what types of charts to pull, it is ultimately their discretion as to what actual charts are inputted. The implication of this is that physicians may not always select charts that accurately represent their typical prescribing behavior. It is our hypothesis that physicians can hold a distorted view of what their “typical” prescribing actually is, or, in some cases, physicians may select charts they feel may be more interesting to the research sponsor or charts that portray their prescribing in an optimal perspective. While selection bias can be mitigated in our respondent instructions, it cannot be completely avoided. As such, we commonly account for this in the analysis through weighting or other techniques.
A multifaceted look
As with any research study, the elements baked into the chart audit design dictate the analysis that can be gleaned from the data. With deliberate planning, chart audit research delivers a multifaceted look at a prescribing environment, illustrating treatment progression from the perspective of the patient, the physician and the disease or condition characteristics.
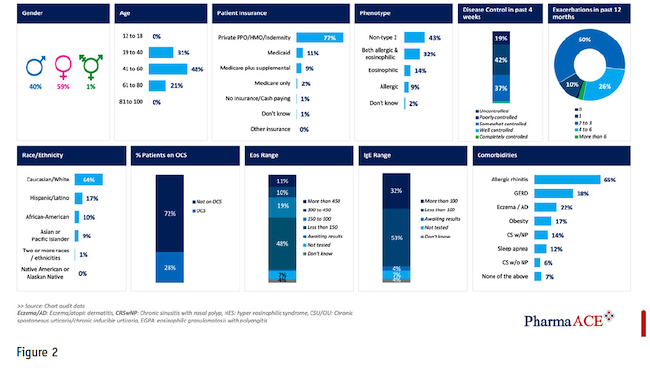
First, from the patient perspective, including elements such as gender, age, geography, insurance type, treatment location or comorbidities allows the analysis to highlight key insights as they relate to patient profiles. For example, analysis can be constructed to show the patient profile most associated with a client’s brand, as well as that associated with key competitors.
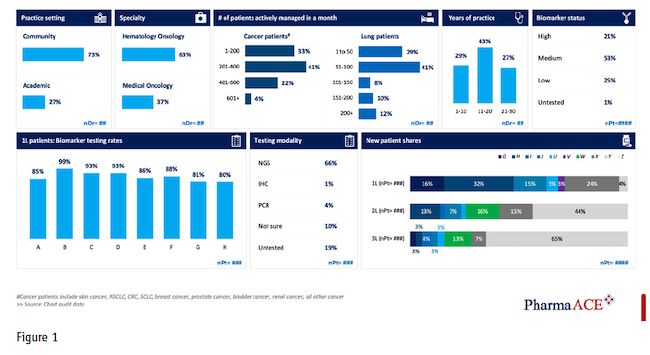
On the physician side, with the correct tactical elements in the chart design, clients can discern the physician characteristics that most embody their prescribers and, equally insightful, those of competitive products. Common physician profile factors include practice setting, specialty, number of patients with the disease in question, years in practice and even metrics such as testing modality. This is potent information to layer onto analysis and becomes even more insightful as physicians state the reasons behind their prescribing decisions. While probing physician motivations is a common tactic in primary research, it takes on an elevated significance when appending to this information actual patient charts rather than recall captured in ATUs or other similar studies.
The third layer to chart audit design that informs analysis is the specific disease and treatment metrics. By extrapolating from patient chart metrics such as diagnosis date, current treatment status, prior treatments and diagnostic testing results, a comprehensive profile of patients can be constructed.
Chart audit analysis enables brand teams to answer key business questions such as how the brand is performing in terms of market share compared to competitors and what is the physician profile prescribing the brand versus competitors. Figure 1 shows a physician dashboard compiled from chart audit data.
Similarly, the patient profiles (Figure 2) developed illustrate those using a brand versus competitors as well as real-world data to support the patient journey among lines of therapy for the brand compared against its competition.
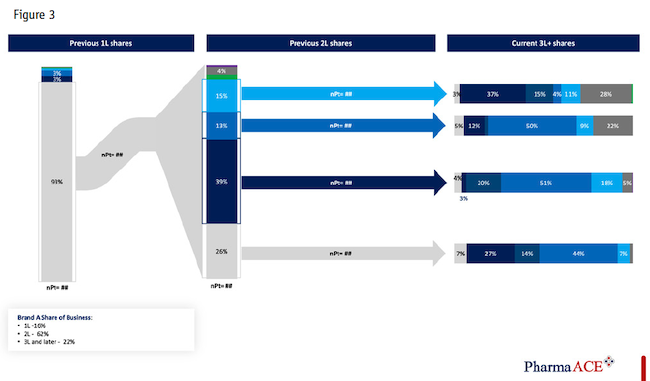
In addition, users of chart audit data can assess: the evolution of treatment algorithms over time; the impact of national treatment guidelines on that algorithm; the reasons for treatment selection, switching and discontinuation; newly launched product adoption and uptake as well as evaluation of target and non-target physician respondents. Figure 3 demonstrates a treatment progression visual common in chart research.
All analysis should be augmented with secondary data to triangulate and supplement brand insights to provide additional value to the brand teams who are most often funding the primary marketing research and secondary data purchasing.
Chart audit outputs can be a PowerPoint report produced periodically or an online report securely shared with the client and relevant stakeholders. Once the format is finalized, reports can be automated and produced showing new-to-brand prescriptions or claims data to further enhance the value for teams who desire early insights, leading indicators of new product launches, new indication launches, competitive launches or the impact of new data releases to physician audiences.
A final note on chart audit research is that, to be most effective, chart audits should remain fluid. One way to ensure that chart audits stay relevant to the brand team is to keep an active feedback loop in place. We characterize this loop in its component parts of fielding feedback, analysis review and client subject matter expertise.
On the fielding side, once an initial wave of a chart audit has been completed, the team can assess the recruitment statistics and data quality. It is important to identify any barriers to participation, i.e., where are physicians disqualifying, and determine if adjustments can be made to increase response while still meeting client goals. Similarly, assessing stumbling blocks in the survey that are causing respondents extra time or confusion is a good research practice.
With respect to analysis, as with any recurring or tracking-type research, it is common for clients to add questions or sections as brands evolve and needs change. It is often less of a priority to eliminate questions no longer serving an analytical purpose. It is helpful to ask: Are there questions in the survey that are no longer necessary for analysis?
As brands evolve, key performance metrics may be adjusted as well and culling questions that do not factor into decision points is vital to prevent the research from becoming overly burdensome for respondents and to maintain a high level of engagement with physician respondents.
To ensure timely subject matter expertise, clients play an integral role in the feedback loop as they are privy to information regarding changes to treatment guidelines, new indications or changes to the competitive product mix. Any updates to the treatment landscape must be replicated in the chart to ensure the instrument collects timely and relevant information.
Aligned with segmentation and targeting
In summary, the chart audit can be a valuable and timely market research tool for brand teams to consider as they are launching a new product or indication as well as tracking an existing or competitive product. Chart audits can assist in providing leading insights to brand teams regarding reasons for treatment selection/switch/discontinuation, sequencing of regimens and profiles of both physicians and patients that can be aligned with internal segmentation and targeting. Integrating your market research analysis and recruiting partner in the process of brand team report readouts and third-party data triangulation is essential for success and enhanced insights to maximize chart audit research value.