Creating a health-literate approach
Editor's note: Lisa R. Courtade is executive director, global customer and brand insights, Merck & Co. Inc. Laurie Myers is director, global health literacy, Merck & Co. Inc.
In seeking to connect more strongly with consumers, as a profession we in marketing research often turn to the next new method, from mobile to text analytics to neuroscience. However, our experience has shown us that there is also opportunity in refining existing approaches to achieve deeper, more meaningful and relevant customer insights. By thinking more broadly about our target health care consumer and including those with a range of health literacy levels, we have been able to improve our methods and deliver communications that are better understood by all audiences.
Nearly nine out of 10 Americans struggle with understanding health-related information. Health literacy is commonly defined as “the degree to which individuals have the capacity to obtain, communicate, process and understand basic health information and services needed to make appropriate health decisions.”1 Low levels of health literacy may span all age, gender, education and income groups. It can also be compounded by the emotional state of patients who are trying to grasp the implications of a new diagnosis. Patients and caregivers who struggle to understand health information have a difficult time following medical directions and are at greater risk for poor health outcomes. Low health literacy is linked to increased hospitalization rates, less frequent screenings for disease, increased rates of disease and mortality and poor adherence to treatment. “Health literacy is a stronger predictor of a person’s health status than age, income, employment status and race.”2
Numerous studies indicate that most health-related information is written beyond the level that the average adult can understand. As the Patient Protection and Affordable Care Act (ACA) extends health insurance coverage to millions of health care consumers,3 more focus is needed to ensure that this growing universe of patients have the information needed to make informed health decisions. For many of these patients, it may be their first time with health insurance coverage and they are just learning to navigate the health care system. Generally, people want to be healthy and want to take care of themselves but they don’t always understand how. In addition to health care providers, pharmaceutical companies have an amazing opportunity to help empower patients to manage their own health through informative communications including patient labeling, educational materials and direct-to-consumer advertising. However, it is critical that companies engage with consumers in a way that is meaningful and understandable.
Until a few years ago, there was little recognition of the need to include respondents with low health literacy; moreover, common recruitment practices tended to underrepresent these populations. Random and convenience sample approaches, even when stratified for education, have generally resulted in the inclusion of few respondents who could be qualified as having limited health literacy. As we’ve learned, individuals with limited health literacy are harder to locate, less likely to participate in marketing research, are often screened out through standard exclusion criteria (such as age) and are not generally represented in recruitment databases.
Apply best practices in health literacy
In 2011, Merck made an organizational commitment to improve health literacy as part of our corporate mission to improve health. As we embarked upon achieving this objective, we partnered with leaders in the field of health literacy at Northwestern and Emory Universities. The goal of this partnership was to apply best practices in health literacy to optimize the development and testing of patient labeling, resulting in improved patient understanding and use. This partnership involved the creation of test materials that applied health literacy principles such as font size, spacing and simple language as well as the inclusion of limited literacy participants.
Very quickly we learned that filling these target samples was not an easy task. These individuals are generally less likely to be in recruitment databases and simply using lower education as a proxy for low health literacy was a poor predictor as it is not necessarily directly correlated. Through the partnership we were able to immediately adopt best practices from health literacy to locate and identify participants for our studies. Key tips we would offer to other researchers would be to:
- expand beyond typical facility lists by recruiting respondents from literacy, community and senior centers;
- offer paper copies of materials to respondents who do not have a computer;
- add a question during screening, “How confident are you filling out forms by yourself?”4;
- use the Newest Vital Sign “ice cream label” assessment during research as a simple and reliable measure of predicting health literacy level, including numeracy skills.5
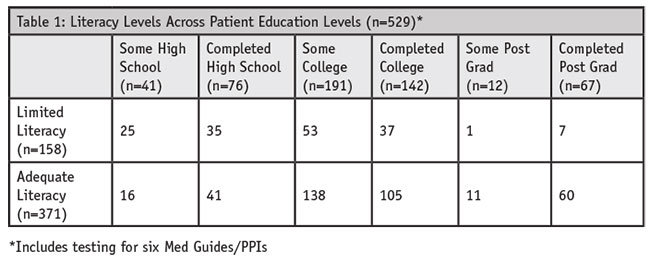
These measures enabled us to expand our sample composition to include a wider range of respondents in-clusive of at least 10 percent to 25 percent low health-literate individuals with a minimal number of screening questions. As evidenced by Table 1 from an assessment of our pilot study results, about 30 percent of respondents had limited literacy. Along the way, we also learned to extend recruiting timelines to allow for nontraditional recruitment.

Provided many insights
The research process itself provided many insights that have become part of the best practices we now follow for testing patient labeling of new molecules. In our early studies, it quickly became evident that we could not simply add respondents with low health literacy to our existing market research methodologies and expect a reliable outcome. The survey-taking behaviors of this audience were notably different, which resulted in frustration for the participant, the interviewer and the client and at times led to inaccurate results. For instance, we observed that respondents with low health literacy often chose the first correct answer they encountered rather than reading through all options in a multiple response list where “all of the above” is an option. Qualitative inquiry demon-strated that respondents understood the information presented, it was the question sequence they struggled with; this resulted in an artificial decrease in overall comprehension scores. It was also painfully apparent that many tasks, including complex message-sorts, were overwhelming for many low health literacy participants. As a result, we have adopted a new practice of conducting a health literacy review to apply multiple best practices from the field of health literacy to not only the documents but also to the tasks and interview guides. Simplified language within the content itself is important but so too were clean layout and typography, descriptive graphics and clear tasks. (For more information see www.iom.edu/global/perspectives/2014/healthliteracyguidance.aspx)
This new, more health-literate approach has proven effective in multiple rounds of patient la-beling research. As demonstrated in Table 2, we have consistently achieved strong comprehension (85 percent or better) among respondents with both limited and adequate health literacy. Health literacy experts agree this development and testing process is an optimal model for the design of clear, well-understood patient labeling.

Early on in our journey, and throughout, there have been questions regarding whether consumers or medical professionals who have advanced degrees would be offended by the everyday language and simple presentations foundational to health-literate communications. This has not been the case. Well-educated respondents have shared that they appreciate the clarity of the information, because often health information is complex and overwhelming, particularly during times of emotional stress. Moreover, it has been noted that the new format is helpful to these more educated audiences as a caretaker of other family members and to physicians in communicating with patients.
Patients should be empowered
As a pharmaceutical company, achieving our mission is about more than discovering the molecules that can help make people well. It’s also about improving people’s capabilities to make healthy choices, manage their therapies and navigate health systems. Patients should be empowered to manage disease through a better understanding of treatments and prescribed medicines. Health literacy is a critical factor in this understanding. Without it, the chances that a patient will correctly use and fully benefit from our discoveries are slim. At a time when patients and family members are increasingly involved in their own care, clear communication at every point along the patient journey, from researching symptoms to seeking diagnosis to managing disease, is a crucial adjunct to the medicines we discover.
We will continue to partner with patients and their caregivers to promote their understanding of their medical conditions or diseases, the reasons they are being treated and the appropriate use of medications and other treatments. Through this work, we have learned that engaging patients across a range of health literacy levels and incorporating their feedback through advancing our marketing research approaches helps us produce clear, ef-fective health communications.
We are currently working to expand this inclusive, simpler approach to other types of consumer market research by ensuring the consistent application of best practices for health literacy in screening and testing across the business. We also continue to work with market research agencies, facilities and recruiters to improve their ability to identify and engage patients with limited health literacy. We are the first to admit that it is not a science yet and each study reveals new things we have not yet thought of or faced.
Viewed as a model
We believe that our health-literate approach to consumer research may be viewed as a model that could be adopted by the FDA, other pharmaceutical companies, other organizations in the business of health care as well as health systems that generate patient-facing communications. In October 2014, we shared our story in a panel presentation, “Addressing the health literacy challenge through 360º collaboration” at the PMRG Institute in New Brunswick, N.J. Compelled by the impact we had with our research process and the importance of our mission, the PMRG has since adopted health literacy as a key advocacy initiative. The goal of the PMRG initiative is to further the education of marketing research practitioners and to evolve our practices as an industry. The authors welcome additional dialogue and ideas. We invite you to join in the cause to grow and change our marketing research insight process to include and enable patients of all levels of health literacy to understand and better manage their health.
REFERENCES
1 U.S. Department of Health and Human Services. Healthy People 2010. Washington, D.C.: U.S. Government Printing Office; 2000.
2 Weiss B.D. Health Literacy and Patient Safety: Help Patients Understand. The American Medical Association (AMA) Foundation and the AMA. May 2007.
3 www.hhs.gov/healthcare/rights
4 Chew et al.: “Validation of screening questions for limited health literacy in a large VA outpatient population,” Journal of General Internal Medicine 23.5 (2008): 561-66.
5 Weiss B.D., Mays, M.Z., Martz, W., Castro, K.M., DeWalt, D.A., Pignone, M.P., Mockbee, J., Hale, F.A.: “Quick assessment of literacy in primary care: the Newest Vital Sign,” Annals of Family Medicine 3.6 (2005): 514-22.